
Abstract
Purpose
To evaluate the capacity of perfusion CT imaging to distinguish between complete and incomplete responders after neoadjuvant chemoradiation therapy for rectal carcinoma, with particular attention to segmentation technique.
Materials and methods
17 patients were evaluated in this prospective IRB-approved study. For each patient, a perfusion CT acquisition was obtained prior to the initiation of chemoradiation, at 1–2 weeks after the start of chemoradiation, and at 12 weeks after the start of chemoradiation therapy. From each dataset, three perfusion parameters were measured, each in two different ways: a region of interest incorporating only “hot spots” of greatest enhancement and whole-tumor measurements.
Results
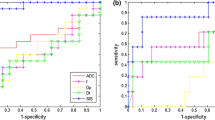
In univariate analysis, blood volume and permeability differed significantly between responders and non-responders. In logistic regression analysis evaluating predictors of the “complete response” outcome, only two predictors were retained as statistically significant: peak hot spot blood volume 1–2 weeks into therapy (OR 10.25, p = 0.0026) and hot spot permeability decline at 12 weeks after the initiation of therapy (OR 5.62, p = 0.03). The overall likelihood ratio test for this model supported the conclusion that hot spot blood volume and hot spot permeability decline were significant predictors of the complete pathologic response outcome (p < 0.0001).
Conclusion
In this pilot study, peak tumor blood volume and decline in tumor permeability, when measured in “hot spots” of greatest enhancement, were strong predictors of complete therapeutic response in rectal cancer after neoadjuvant therapy.


Similar content being viewed by others


References
Sauer R, Becker H, Hohenberger W, et al. (2004) Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 351:1731–1740
Sauer R, Liersch T, Merkel S, et al. (2012) Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol 30:1926–1933
van der Paardt MP, Zagers MB, Beets-Tan RG, Stoker J, Bipat S (2013) Patients who undergo preoperative chemoradiotherapy for locally advanced rectal cancer restaged by using diagnostic MR imaging: a systematic review and meta-analysis. Radiology 269:101–112
Glynne-Jones R, Hughes R (2016) Complete response after chemoradiotherapy in rectal cancer (watch-and-wait): have we cracked the code? Clin Oncol 28:152–160
Smith JJ, Chow OS, Gollub MJ, et al. (2015) Organ Preservation in Rectal Adenocarcinoma: a phase II randomized controlled trial evaluating 3-year disease-free survival in patients with locally advanced rectal cancer treated with chemoradiation plus induction or consolidation chemotherapy, and total mesorectal excision or nonoperative management. BMC Cancer 15:767
Prezzi D, Khan A, Goh V (2015) Perfusion CT imaging of treatment response in oncology. Eur J Radiol 884(12):2380–2385
Bellomi M, Rizzo S, Travaini LL, et al. (2007) Role of multidetector CT and FDG-PET/CT in the diagnosis of local and distant recurrence of resected rectal cancer. Radiol Med 112:681–690
Sahani DV, Kalva SP, Hamberg LM, et al. (2005) Assessing tumor perfusion and treatment response in rectal cancer with multisection CT: initial observations. Radiology 234:785–792
Goh V, Shastry M, Engledow A, et al. (2011) Commercial software upgrades may significantly alter Perfusion CT parameter values in colorectal cancer. Eur Radiol 21:744–749
Meier P, Zierler KL (1954) On the theory of the indicator-dilution method for measurement of blood flow and volume. J Appl Physiol 6:731–744
Axel L (1980) Cerebral blood flow determination by rapid-sequence computed tomography: theoretical analysis. Radiology 137:679–686
Axel L (1983) Tissue mean transit time from dynamic computed tomography by a simple deconvolution technique. Invest Radiol 18:94–99
Ostergaard L, Weisskoff RM, Chesler DA, Gyldensted C, Rosen BR (1996) High resolution measurement of cerebral blood flow using intravascular tracer bolus passages. Part I: mathematical approach and statistical analysis. Magn Reson Med 36:715–725
Cancer Colon and Rectum Cancer Staging American Joint Committee on Cancer 7th Edition. Accessed 25 May 2016, at http://cancerstaging.org/references-tools/quickreferences/documents/colonmedium.pdf.
Perez RO, Pereira DD, Proscurshim I, et al. (2009) Lymph node size in rectal cancer following neoadjuvant chemoradiation–can we rely on radiologic nodal staging after chemoradiation? Dis Colon Rectum 52:1278–1284
Janssen MH, Aerts HJ, Kierkels RG, et al. (2010) Tumor perfusion increases during hypofractionated short-course radiotherapy in rectal cancer: sequential perfusion-CT findings. Radiother Oncol 94:156–160
Maas M, Beets-Tan RG, Lambregts DM, et al. (2011) Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer. J Clin Oncol 29:4633–4640
Hayano K, Shuto K, Koda K, et al. (2009) Quantitative measurement of blood flow using perfusion CT for assessing clinicopathologic features and prognosis in patients with rectal cancer. Dis Colon Rectum 52:1624–1629
Goh V, Halligan S, Wellsted DM, Bartram CI (2009) Can perfusion CT assessment of primary colorectal adenocarcinoma blood flow at staging predict for subsequent metastatic disease? A pilot study. Eur Radiol 19:79–89
Fischer MA, Vrugt B, Alkadhi H, et al. (2014) Integrated (1)(8)F-FDG PET/perfusion CT for the monitoring of neoadjuvant chemoradiotherapy in rectal carcinoma: correlation with histopathology. Eur J Nucl Med Mol Imaging 41:1563–1573
Fajardo LF (2005) The pathology of ionizing radiation as defined by morphologic patterns. Acta Oncol 44:13–22
Rodemann HP, Blaese MA (2007) Responses of normal cells to ionizing radiation. Semin Radiat Oncol 17:81–88
Goh V, Halligan S, Gharpuray A, et al. (2008) Quantitative assessment of colorectal cancer tumor vascular parameters by using perfusion CT: influence of tumor region of interest. Radiology 247:726–732
Blazic IM, Lilic GB, Gajic MM. Quantitative assessment of rectal cancer response to neoadjuvant combined chemotherapy and radiation therapy: comparison of three methods of positioning region of interest for ADC measurements at diffusion-weighted MR imaging. Radiology 2016:151908.
Curvo-Semedo L, Portilha MA, Ruivo C, et al. (2012) Usefulness of perfusion CT to assess response to neoadjuvant combined chemoradiotherapy in patients with locally advanced rectal cancer. Acad Radiol 19:203–213
Sanghera B, Banerjee D, Khan A, et al. (2012) Reproducibility of 2D and 3D fractal analysis techniques for the assessment of spatial heterogeneity of regional blood flow in rectal cancer. Radiology 263:865–873
Martens MH, Subhani S, Heijnen LA, et al. (2015) Can perfusion MRI predict response to preoperative treatment in rectal cancer? Radiother Oncol 114:218–223
Bosset JF, Calais G, Mineur L, et al. (2005) Enhanced tumorocidal effect of chemotherapy with preoperative radiotherapy for rectal cancer: preliminary results–EORTC 22921. J Clin Oncol 23:5620–5627
Bosset JF, Collette L, Calais G, et al. (2006) Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med 355:1114–1123
de Campos-Lobato LF, Stocchi L, da Luz Moreira A, et al. (2011) Pathologic complete response after neoadjuvant treatment for rectal cancer decreases distant recurrence and could eradicate local recurrence. Ann Surg Oncol 18:1590–1598
Acknowledgements
The authors would like to thank Ulrike Haberland, PhD for technical input and Robert Berger, RT for image acquisition.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was partially funded by the Society of Abdominal Radiology Wylie J. Dodds Research Award and by the Developmental Cancer Research Award, Stanford Cancer Center Translational Research.
Conflict of interest
Heiko Schmiedeskamp, PhD, is employee of Siemens Healthcare, Dominik Fleischmann, MD, received research support from General Electric Healthcare and Siemens Medical Solutions. The other authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. IRB approval was obtained for this study (IRB protocol #19224, Stanford University).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Kino, A., Shaffer, J., Maturen, K.E. et al. Perfusion CT measurements predict tumor response in rectal carcinoma. Abdom Radiol 42, 1132–1140 (2017). https://doi.org/10.1007/s00261-016-0983-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-016-0983-5