
Immunogenicity of ChAdOx1 nCoV-19 Booster Vaccination Following Two CoronaVac Shots in Healthcare Workers

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Serological Analysis for Humoral and Cellular Immune Responses
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Participants
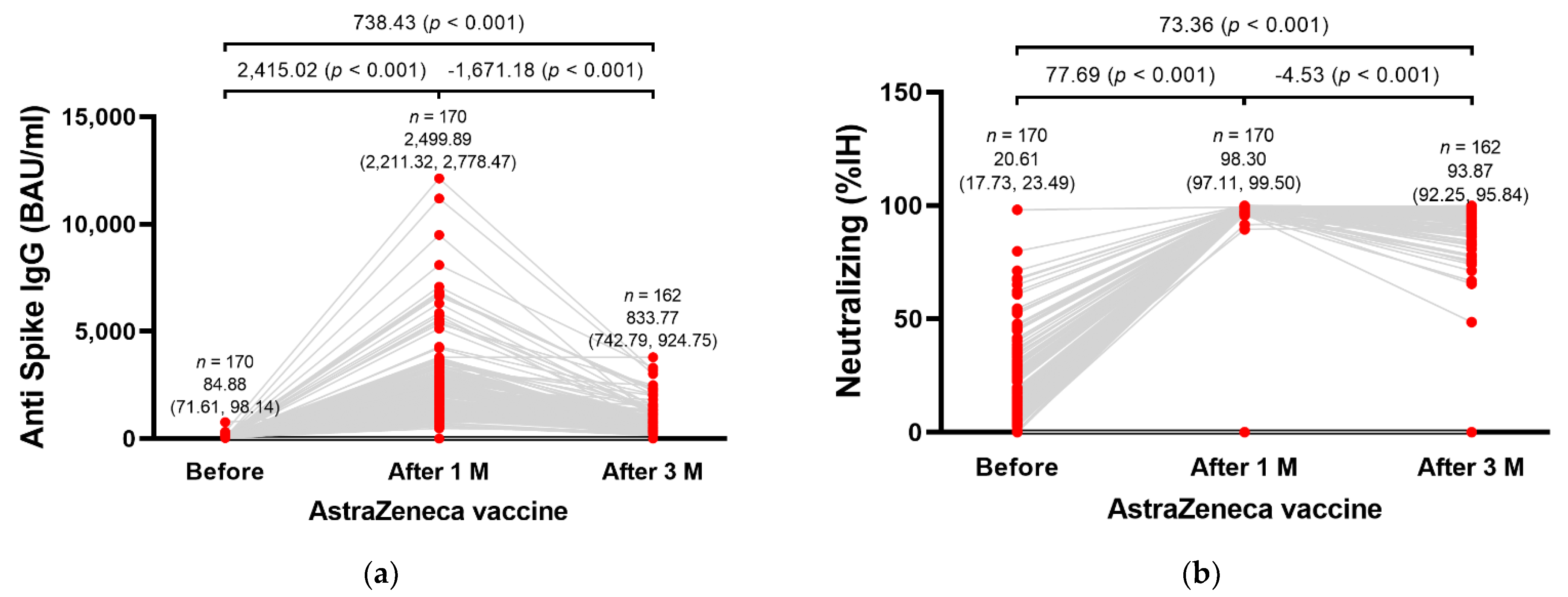
3.2. Humoral Immunogenicity
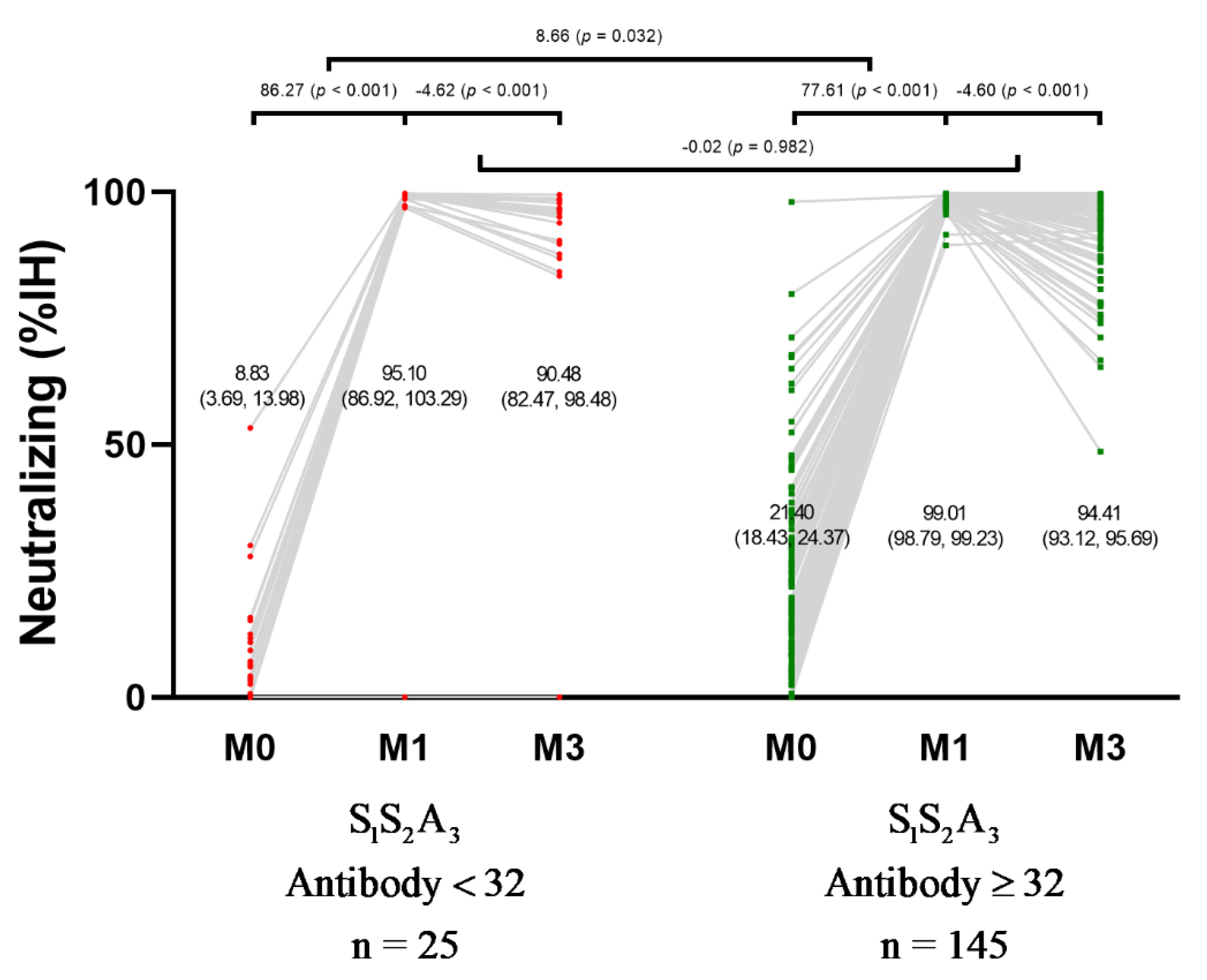
3.3. Humoral Immunogenicity Based on the Baseline Anti-Spike IgG Antibody Level
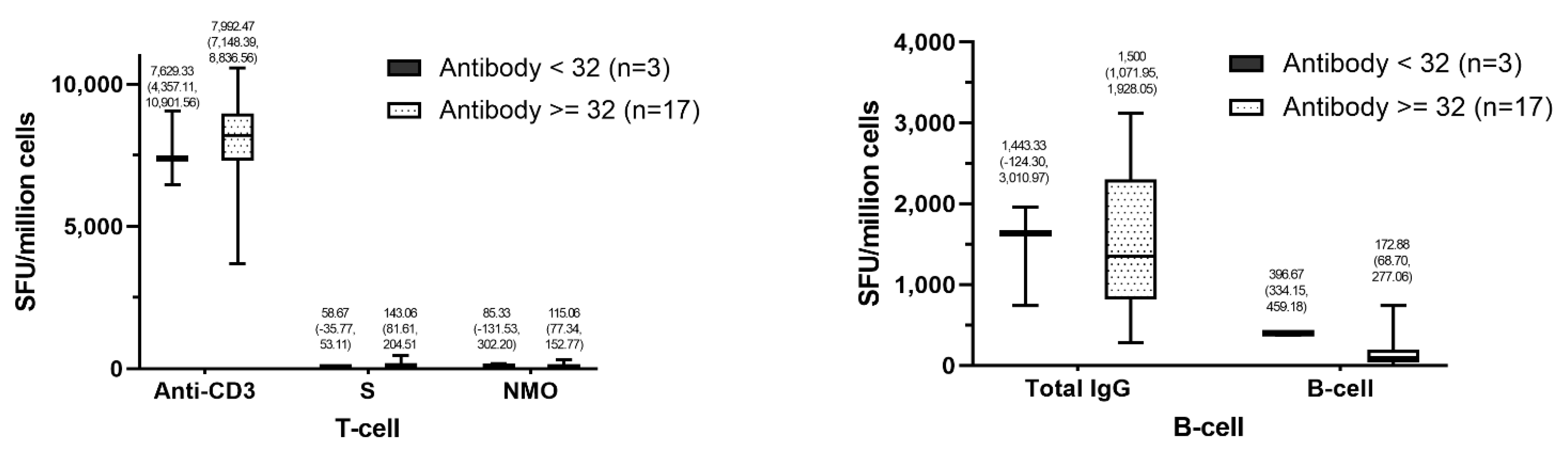
3.4. Cellular Immunogenicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in wuhan, china. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Faller, E.; Wyse, A.; Barry, R.; Conlon, K.; Everard, C.; Finnegan, P.; Foran, C.; Herlihy, E.; Kerr, G.; Lapthorne, S.; et al. Seroprevalence study of SARS-CoV-2 antibodies in healthcare workers following the first wave of the COVID-19 pandemic in a tertiary-level hospital in the south of ireland. BMJ Open 2021, 11, e051415. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, X.; He, J. Challenges to the system of reserve medical supplies for public health emergencies: Reflections on the outbreak of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) epidemic in china. Biosci. Trends 2020, 14, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, L.; Drew, D.; Graham, M.; Joshi, A.; Guo, C.; Ma, W.; Mehta, R.; Warner, E.; Sikavi, D.; Lo, C.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Barrett, E.; Horton, D.; Roy, J.; Gennaro, M.; Brooks, A.; Tischfield, J.; Greenberg, P.; Andrews, T.; Jagpal, S.; Reilly, N.; et al. Prevalence of SARS-CoV-2 infection in previously undiagnosed health care workers in new jersey, at the onset of the U.S. COVID-19 pandemic. BMC Infect. Dis. 2020, 20, 853. [Google Scholar] [CrossRef]
- Nopsopon, T.; Pongpirul, K.; Chotirosniramit, K.; Jakaew, W.; Kaewwijit, C.; Kanchana, S.; Hiransuthikul, N. Seroprevalence of hospital staff in a province with zero COVID-19 cases. PLoS ONE 2021, 16, e0238088. [Google Scholar] [CrossRef]
- Nopsopon, T.; Pongpirul, K.; Chotirosniramit, K.; Hiransuthikul, N. COVID-19 seroprevalence among hospital staff and preprocedural patients in thai community hospitals: A cross-sectional study. BMJ Open 2021, 11, e046676. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Wu, Z.; Hu, Y.; Xu, M.; Chen, Z.; Yang, W.; Jiang, Z.; Li, M.; Jin, H.; Cui, G.; Chen, P.; et al. “Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (coronavac) in healthy adults aged 60 years and older: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial”. Lancet Infect. Dis. 2021, 21, 803–812. [Google Scholar] [CrossRef]
- Benjamanukul, S.; Traiyan, S.; Yorsaeng, R.; Vichaiwattana, P.; Sudhinaraset, N.; Wanlapakorn, N.; Poovorawan, Y. Safety and immunogenicity of inactivated COVID-19 vaccine in health care workers. J. Med. Virol. 2021, 27458, 1–8. [Google Scholar] [CrossRef]
- Mok, C.; Cohen, C.; Cheng, S.; Chen, C.; Kwok, K.; Yiu, K.; Chan, T.; Bull, M.; Ling, K.; Dai, Z.; et al. Comparison of the immunogenicity of bnt162b2 and coronavac COVID-19 vaccines in hong kong. Respirology 2021, 14191, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sauré, D.; O’Ryan, M.; Torres, J.; Zuniga, M.; Santelices, E.; Basso, L. Dynamic igg seropositivity after rollout of coronavac and bnt162b2 COVID-19 vaccines in chile: A sentinel surveillance study. Lancet Infect. Dis. 2021, 22, 56–63. [Google Scholar] [CrossRef]
- Yigit, M.; Ozkaya-Parlakay, A.; Cosgun, Y.; Ince, Y.; Bulut, Y.; Senel, E. Should a third booster dose be scheduled after two doses of coronavac? A single-center experience. J. Med. Virol. 2022, 94, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Zeng, G.; Wu, Q.; Pan, H.; Li, M.; Yang, J.; Wang, L.; Wu, Z.; Jiang, D.; Deng, X.; Chu, K.; et al. Immunogenicity and safety of a third dose of coronavac, and immune persistence of a two-dose schedule, in healthy adults: Interim results from two single-centre, double-blind, randomised, placebo-controlled phase 2 clinical trials. Lancet Infect. Dis. 2021, 21, 1–13. [Google Scholar] [CrossRef]
- Keskin, A.; Bolukcu, S.; Ciragil, P.; Topkaya, A. SARS-CoV-2 specific antibody responses after third coronavac or bnt162b2 vaccine following two-dose coronavac vaccine regimen. J. Med. Virol. 2022, 94, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Soytas, R.; Cengiz, M.; Islamoglu, M.; Uysal, B.; Yavuzer, S.; Yavuzer, H. Antibody responses to COVID-19 vaccines in older adults. J. Med. Virol. 2021, 27531, 1–5. [Google Scholar] [CrossRef]
- Vacharathit, V.; Aiewsakun, P.; Manopwisedjaroen, S.; Srisaowakarn, C.; Laopanupong, T.; Ludowyke, N.; Phuphuakrat, A.; Setthaudom, C.; Ekronarongchai, S.; Srichatrapimuk, S.; et al. Coronavac induces lower neutralising activity against variants of concern than natural infection. Lancet Infect. Dis. 2021, 21, 1352–1354. [Google Scholar] [CrossRef]
- Chen, Y.; Shen, H.; Huang, R.; Tong, X.; Wu, C. Serum neutralising activity against SARS-CoV-2 variants elicited by coronavac. Lancet Infect. Dis. 2021, 21, 1071–1072. [Google Scholar] [CrossRef]
- Flaxman, A.; Marchevsky, N.; Jenkin, D.; Aboagye, J.; Aley, P.; Angus, B.; Belij-Rammerstorfer, S.; Bibi, S.; Bittaye, M.; Cappuccini, F.; et al. Reactogenicity and immunogenicity after a late second dose or a third dose of chadox1 ncov-19 in the uk: A substudy of two randomised controlled trials (cov001 and cov002). Lancet 2021, 398, 981–990. [Google Scholar] [CrossRef]
- Munro, A.; Janani, L.; Cornelius, V.; Aley, P.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of chadox1 ncov-19 or bnt162b2 in the uk (cov-boost): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Assawasaksakul, T.; Sathitratanacheewin, S.; Vichaiwattana, P.; Wanlapakorn, N.; Poovorawan, Y.; Kittanamongkolchai, W. Immunogenicity, safety and reactogenicity of a heterogeneous booster following the coronavac inactivated SARS-CoV-2 vaccine in patients with sle: A case series. RMD Open 2021, 7, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Yorsaeng, R.; Suntronwong, N.; Phowatthanasathian, H.; Assawakosri, S.; Kanokudom, S.; Thongmee, T.; Vichaiwattana, P.; Auphimai, C.; Wongsrisang, L.; Srimuan, D.; et al. Immunogenicity of a third dose viral-vectored COVID-19 vaccine after receiving two-dose inactivated vaccines in healthy adults. Vaccine 2021, 40, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Singhatiraj, E.; Pongpirul, K.; Jongkaewwattana, A.; Hirankarn, N. Intradermal chadox1 vaccine following two coronavac shots: A case report. Vaccines 2021, 9, 990. [Google Scholar] [CrossRef] [PubMed]
- Ongkittikul, S.; Rompho, P. SARS-CoV-2 igg antibody response after immunization of healthcare workers with inactivated COVID-19 vaccine (coronavac) at phyathai 3 hospital. Bangk. Med. J. 2021, 17. Available online: https://he02.tci-thaijo.org/index.php/bkkmedj/article/view/251091 (accessed on 21 December 2021). [CrossRef]
- Angkasekwinai, N.; Sewatanon, J.; Niyomnaitham, S.; Phumiamorn, S.; Sukapirom, K.; Sapsutthipas, S.; Sirijatuphat, R.; Wittawatmongkol, O.; Senawong, S.; Mahasirimongkol, S.; et al. Safety and immunogenicity of coronavac and chadox1 against the SARS-CoV-2 circulating variants of concern (alpha, delta, beta) in thai healthcare workers. medRxiv 2021, 21264451, 1–28. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total |
|---|---|
| Age (years) | |
| 18–25 | 8 (4.71%) |
| 26–30 | 18 (10.59%) |
| 31–35 | 19 (11.18%) |
| 36–40 | 22 (12.94%) |
| 41–45 | 19 (11.18%) |
| 46–50 | 33 (19.41%) |
| 51–55 | 26 (15.29%) |
| 56–60 | 25 (14.71%) |
| Female | 138 (81.81%) |
| Smoking | 8 (4.71%) |
| Comorbidities | 72 (42.35%) |
| History of Vaccine Allergy | 2 (1.18%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prasithsirikul, W.; Pongpirul, K.; Nopsopon, T.; Phutrakool, P.; Pongpirul, W.; Samuthpongtorn, C.; Suwanwattana, P.; Jongkaewwattana, A. Immunogenicity of ChAdOx1 nCoV-19 Booster Vaccination Following Two CoronaVac Shots in Healthcare Workers. Vaccines 2022, 10, 217. https://doi.org/10.3390/vaccines10020217
Prasithsirikul W, Pongpirul K, Nopsopon T, Phutrakool P, Pongpirul W, Samuthpongtorn C, Suwanwattana P, Jongkaewwattana A. Immunogenicity of ChAdOx1 nCoV-19 Booster Vaccination Following Two CoronaVac Shots in Healthcare Workers. Vaccines. 2022; 10(2):217. https://doi.org/10.3390/vaccines10020217
Chicago/Turabian StylePrasithsirikul, Wisit, Krit Pongpirul, Tanawin Nopsopon, Phanupong Phutrakool, Wannarat Pongpirul, Chatpol Samuthpongtorn, Pawita Suwanwattana, and Anan Jongkaewwattana. 2022. "Immunogenicity of ChAdOx1 nCoV-19 Booster Vaccination Following Two CoronaVac Shots in Healthcare Workers" Vaccines 10, no. 2: 217. https://doi.org/10.3390/vaccines10020217