
Establishing Healthcare Worker Performance and Safety in Providing Critical Care for Patients in a Simulated Ebola Treatment Unit: Non-Randomized Pilot Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
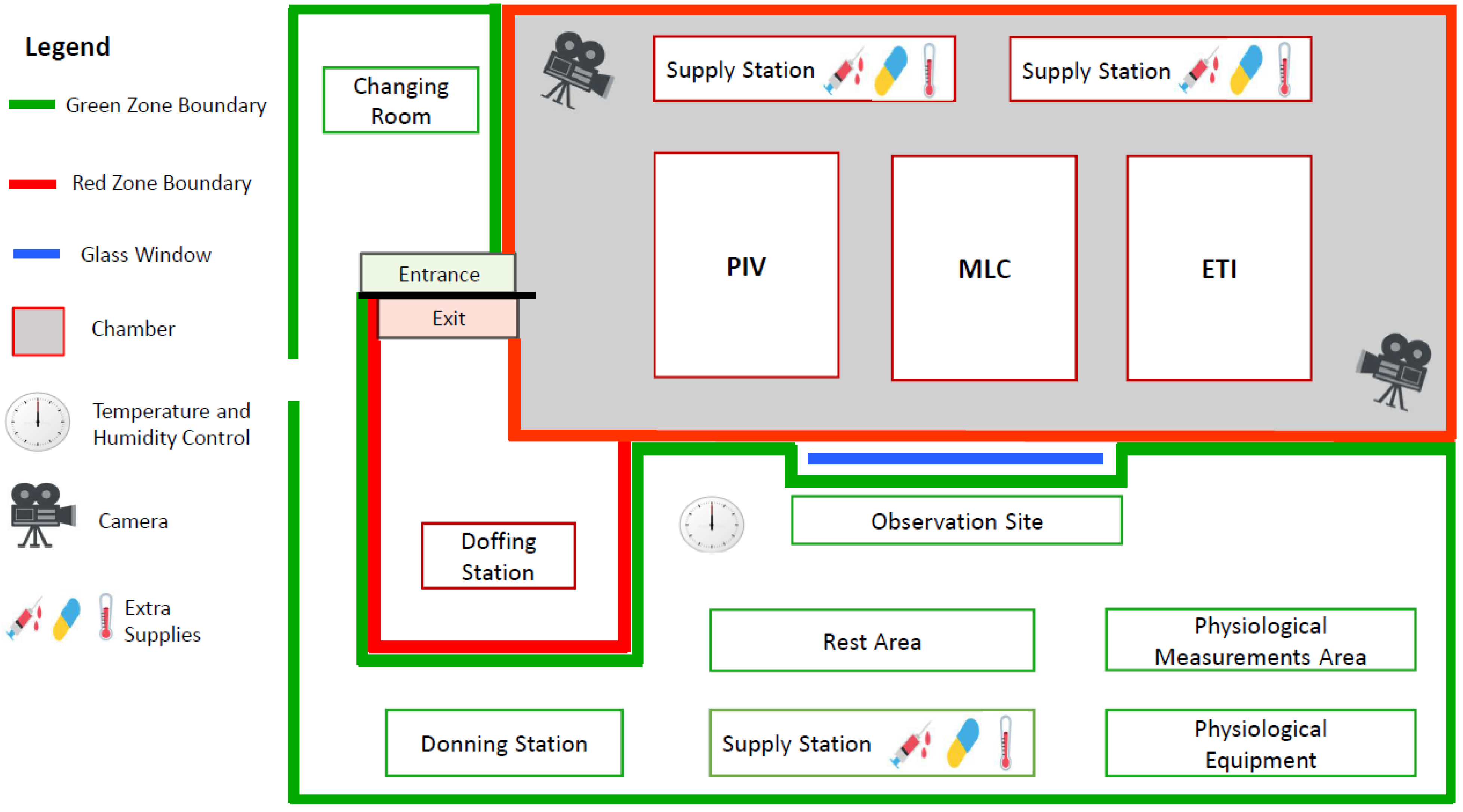
2.2. Study Setting
2.3. Study Population
2.4. Study Materials
2.5. Procedures
2.5.1. Participant Orientation
2.5.2. Participant Monitoring
2.5.3. Chamber and Post-Chamber Procedures
2.6. Outcome Definitions
2.6.1. Task Performance
2.6.2. Participant Safety
2.6.3. Self-Reported Feasibility and Safety
2.7. Data Management and Statistical Analysis
3. Results
3.1. Participant Demographics and Baseline Characteristics
3.2. Chamber Settings
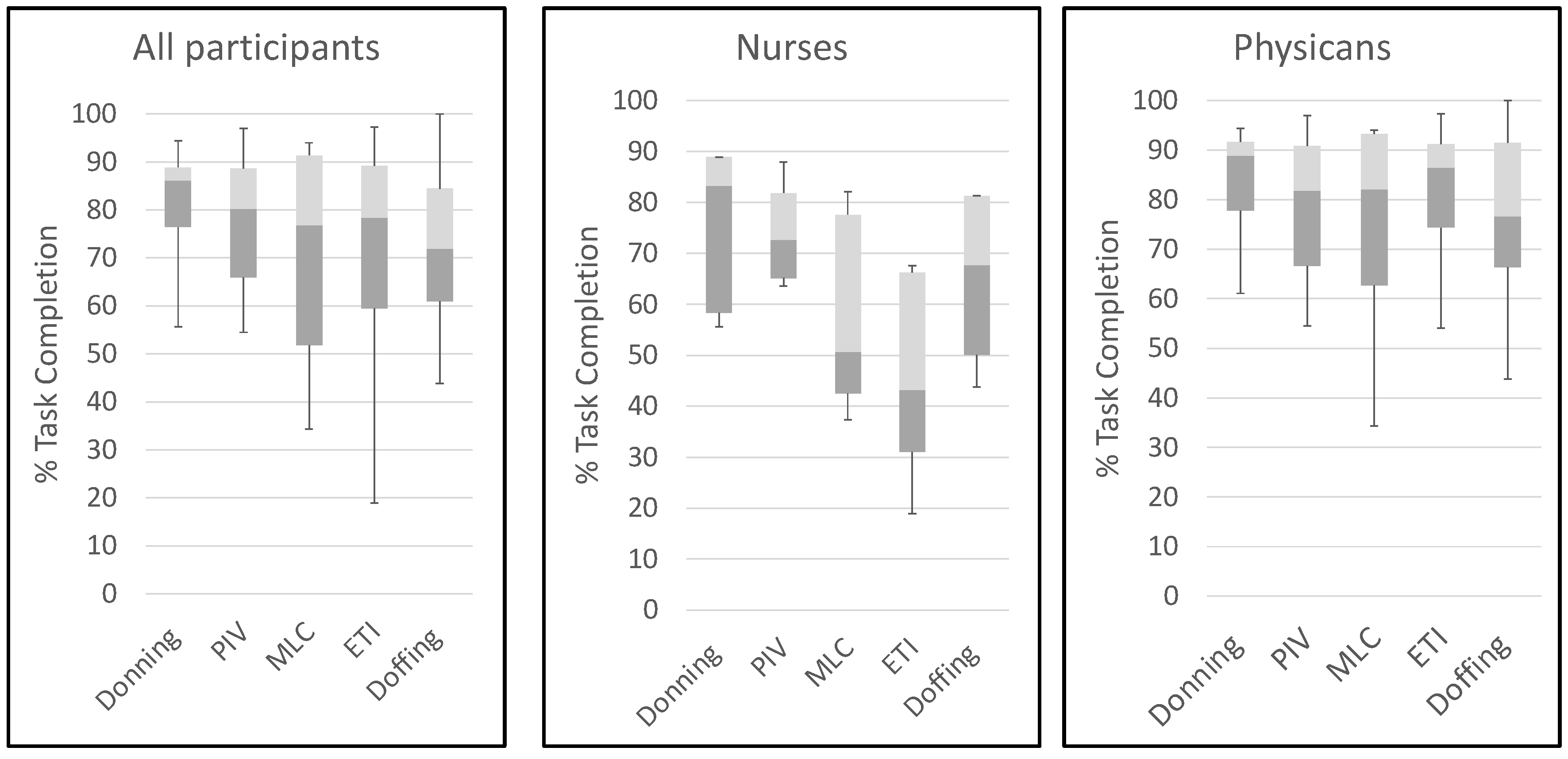
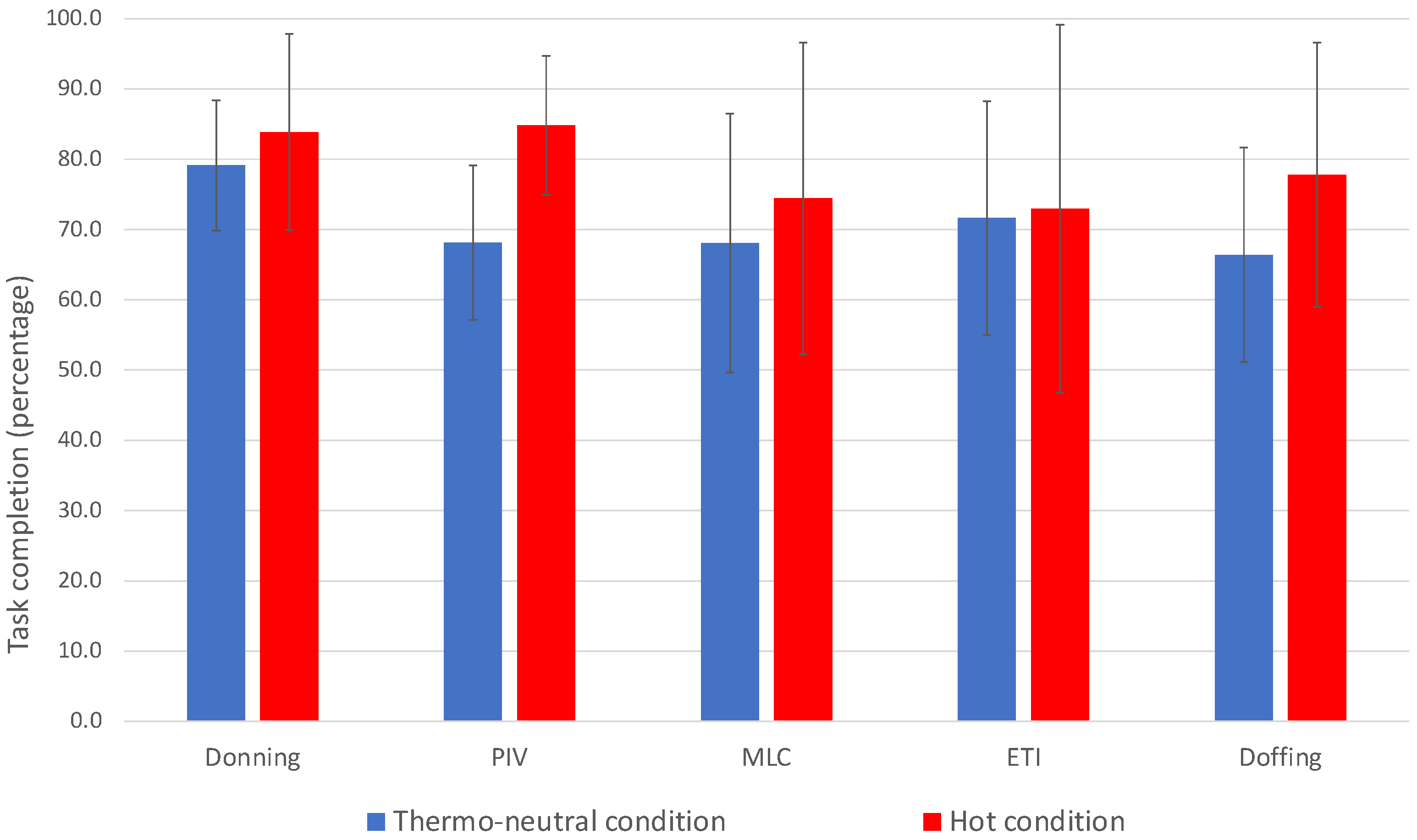
3.3. Task Performance
3.4. Self-Reported Symptoms and Concerns
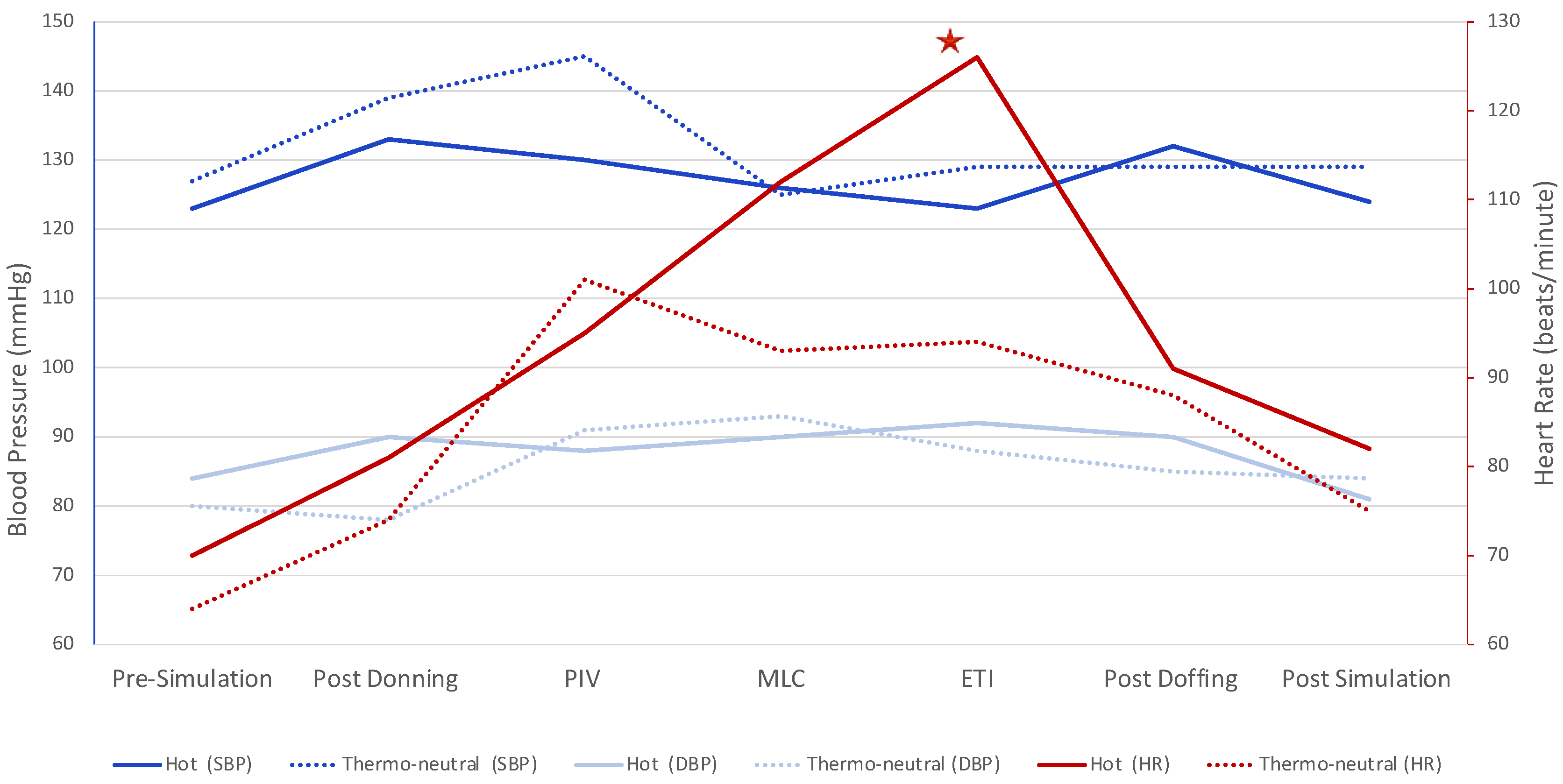
3.5. Participant Safety
3.6. Protocol Changes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bah, E.I.; Lamah, M.C.; Fletcher, T.; Jacob, S.T.; Brett-Major, D.M.; Sall, A.A.; Shindo, N.; Fischer, W.A., II; Lamontagne, F.; Saliou, S.M.; et al. Clinical presentation of patients with Ebola virus disease in Conakry, Guinea. N. Engl. J. Med. 2015, 372, 40–47. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Ebola Virus Disease [Fact Sheet 23 February 2021]. Available online: https://www.who.int/news-room/fact-sheets/detail/ebola-virus-disease (accessed on 28 October 2021).
- World Health Organization. Ebola in the Democratic Republic of the Congo: Health Emergency Update. Available online: https://www.who.int/emergencies/diseases/ebola/drc-2019 (accessed on 27 November 2019).
- Parpia, A.S.; Ndeffo-Mbah, M.L.; Wenzel, N.S.; Galvani, A.P. Effects of Response to 2014-2015 Ebola Outbreak on Deaths from Malaria, HIV/AIDS, and Tuberculosis, West Africa. Emerg. Infect. Dis. 2016, 22, 433–441. [Google Scholar] [CrossRef]
- Henao-Restrepo, A.M.; Camacho, A.; Longini, I.M.; Watson, C.H.; Edmunds, W.J.; Egger, M.; Carroll, M.W.; Dean, N.E.; Diatta, I.; Doumbia, M.; et al. Efficacy and effectiveness of an rVSV-vectored vaccine in preventing Ebola virus disease: Final results from the Guinea ring vaccination, open-label, cluster-randomised trial (Ebola Ca Suffit!). Lancet 2017, 389, 505–518. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Adhikari, N.K.J.; Kwon, H.Y.; Teo, K.; Siemieniuk, R.; Lamontagne, F.; Chan, A.; Mishra, S.; Murthy, S.; Kiiza, P.; et al. Anti-Ebola therapy for patients with Ebola virus disease: A systematic review. BMC Infect. Dis. 2019, 19, 376. [Google Scholar] [CrossRef] [PubMed]
- Mulangu, S.; Dodd, L.E.; Davey, R.T., Jr.; Tshiani Mbaya, O.; Proschan, M.; Mukadi, D.; Lusakibanza Manzo, M.; Nzolo, D.; Tshomba Oloma, A.; Ibanda, A.; et al. PALM Consortium Study Team, A Randomized, Controlled Trial of Ebola Virus Disease Therapeutics. N. Engl. J. Med. 2019, 381, 2293–2303. [Google Scholar] [CrossRef]
- Uyeki, T.M.; Mehta, A.K.; Davey, R.T., Jr.; Liddell, A.M.; Wolf, T.; Vetter, P.; Schmiedel, S.; Grunewald, T.; Jacobs, M.; Arribas, J.R.; et al. European Clinical Network on Clinical Management of Ebola Virus Disease Patients in the U.S. and Europe, Clinical Management of Ebola Virus Disease in the United States and Europe. N. Engl. J. Med. 2016, 374, 636–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickson, S.J.; Clay, K.A.; Adam, M.; Ardley, C.; Bailey, M.S.; Burns, D.S.; Cox, A.T.; Craig, D.G.; Espina, M.; Ewington, I.; et al. Enhanced case management can be delivered for patients with EVD in Africa: Experience from a UK military Ebola treatment centre in Sierra Leone. J. Infect. 2018, 76, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Langer, M.; Portella, G.; Finazzi, S.; Chatenoud, L.; Lanini, S.; Vairo, F.; Fowler, R.; Miccio, R.; Ippolito, G.; Bertolini, G.; et al. Intensive care support and clinical outcomes of patients with Ebola virus disease (EVD) in West Africa. Intensive Care Med. 2018, 44, 1266–1275. [Google Scholar] [CrossRef] [Green Version]
- Lamontagne, F.; Fowler, R.A.; Adhikari, N.K.; Murthy, S.; Brett-Major, D.M.; Jacobs, M.; Uyeki, T.M.; Vallenas, C.; Norris, S.L.; Fischer, W.A., II; et al. Evidence-based guidelines for supportive care of patients with Ebola virus disease. Lancet 2018, 391, 700–708. [Google Scholar] [CrossRef] [Green Version]
- Grillet, G.; Marjanovic, N.; Diverrez, J.M.; Tattevin, P.; Tadie, J.M.; L′Her, E. Intensive care medical procedures are more complicated, more stressful, and less comfortable with Ebola personal protective equipment: A simulation study. J. Infect. 2015, 71, 703–706. [Google Scholar] [CrossRef]
- Grelot, L.; Koulibaly, F.; Maugey, N.; Janvier, F.; Foissaud, V.; Aletti, M.; Savini, H.; Cotte, J.; Dampierre, H.; Granier, H.; et al. Moderate Thermal Strain in Healthcare Workers Wearing Personal Protective Equipment During Treatment and Care Activities in the Context of the 2014 Ebola Virus Disease Outbreak. J. Infect. Dis. 2016, 213, 1462–1465. [Google Scholar] [CrossRef] [Green Version]
- Maynard, S.L.; Kao, R.; Craig, D.G. Impact of personal protective equipment on clinical output and perceived exertion. J. R. Army Med. Corps 2016, 162, 180–183. [Google Scholar] [CrossRef]
- Mazlomi, A.; Golbabaei, F.; Farhang Dehghan, S.; Abbasinia, M.; Mahmoud Khani, S.; Ansari, M.; Hosseini, M. The influence of occupational heat exposure on cognitive performance and blood level of stress hormones: A field study report. Int. J. Occup. Saf. Ergon. 2017, 23, 431–439. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Lancaster, G.A.; Campbell, M.J.; Thabane, L.; Hopewell, S.; Coleman, C.L.; Bond, C.M. Defining Feasibility and Pilot Studies in Preparation for Randomised Controlled Trials: Development of a Conceptual Framework. PLoS ONE 2016, 11, e0150205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Clinical Management of Patients with Viral Haemorrhagic Fever: A Pocket Guide for the Front-Line Health Worker; World Health Organization: Geneva, Switzerland, 2016; p. 203. [Google Scholar]
- Kiiza, P.; Adhikari, N.K.J.; Mullin, S.; Teo, K.; Fowler, R.A. Principles and Practices of Establishing a Hospital-Based Ebola Treatment Unit. Crit. Care Clin. 2019, 35, 697–710. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Jamnik, V.K.; Bredin, S.S.D.; Gledhill, N. PAR-Q+ Research Collaboration, The Physical Activity Readiness Questionnaire (PAR-Q+) and electronic Physical Activity Readiness Medical Examination (ePARmed-X+). Health Fit. J. Can. 2011, 4, 3–23. [Google Scholar]
- World Health Organization. How to Put On and How to Remove Personal Protective Equipment—Posters. Available online: https://www.who.int/csr/resources/publications/ebola/ppe-steps/en/ (accessed on 3 September 2019).
- Hollies, N.R.; Custer, A.G.; Morin, C.J.; Howard, M.E. A human perception analysis approach to clothing comfort. Text. Res. J. 1979, 49, 557–564. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guidelines for the Safe Transport of Infectious Substances and Diagnostic Specimens. Available online: https://www.who.int/csr/emc97_3.pdf (accessed on 28 October 2021).
- Centers for Disease Control and Prevention. Guidance for Collection, Transport and Submission of Specimens for Ebola Virus Testing. Available online: https://www.cdc.gov/vhf/ebola/laboratory-personnel/specimens.html (accessed on 28 October 2021).
- Likert, R. A technique for the measurement of attitudes. Arch. Psychol. 1932, 22, 5–55. [Google Scholar]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Potter, A.W.; Gonzalez, J.A.; Xu, X. Ebola Response: Modeling the Risk of Heat Stress from Personal Protective Clothing. PLoS ONE 2015, 10, e0143461. [Google Scholar] [CrossRef] [Green Version]
- Taylor, L.; Watkins, S.L.; Marshall, H.; Dascombe, B.J.; Foster, J. The Impact of Different Environmental Conditions on Cognitive Function: A Focused Review. Front. Physiol. 2015, 6, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbeek, J.H.; Rajamaki, B.; Ijaz, S.; Tikka, C.; Ruotsalainen, J.H.; Edmond, M.B.; Sauni, R.; Kilinc Balci, F.S. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst. Rev. 2019, 7, CD011621. [Google Scholar] [CrossRef] [PubMed]
- Curtis, H.A.; Trang, K.; Chason, K.W.; Biddinger, P.D. Video-Based Learning vs Traditional Lecture for Instructing Emergency Medicine Residents in Disaster Medicine Principles of Mass Triage, Decontamination, and Personal Protective Equipment. Prehosp. Disaster Med. 2018, 33, 7–12. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n = 18 |
|---|---|
| Age, years, mean (SD) | 40 (7) |
| Body mass index, kg/m2, mean (SD), n (%) | 24.5 (5.8) |
| <25 | 11 (61.1) |
| 25–29.9 | 6 (33.3) |
| ≥30 | 1 (5.6) |
| Sex, Female, n (%) | 9 (50) |
| Profession,n (%) | |
| Nurse | 5 (27.8) |
| Physician | 13 (72.2) |
| Clinical specialty,n (%) | |
| Critical Care | 12 (66.6) |
| Emergency Medicine | 3 (16.7) |
| Other in-patient care | 3 (16.7) |
| Work experience, years, n (%) (n = 16) | |
| <10 | 7 (43.8) |
| 10–20 | 6 (37.4) |
| >20 | 3 (18.8) |
| Work experience in an ETU, n (%) | 2 (11.1) |
| Work experience in austere environments, n (%) | 11 (61.1) |
| Prior procedural experience,n (%) | |
| Peripheral intravenous catheter insertion (n = 17) | 14 (82.4) |
| Midline catheter insertion (n = 17) | 6 (35.3) |
| Central venous catheter insertion (n = 17) | 14 (82.4) |
| Endotracheal intubation (n = 17) | 14 (82.4) |
| Triple packaging of blood samples (n = 15) | 4 (26.7) |
| Total Time in Chamber (n = 18) | PIV Catheter (n = 18) | Midline Catheter (n = 17) | Endotracheal Intubation (n = 17) | |
|---|---|---|---|---|
| All | 68.5 (10.3) | 15.7 (5.7) | 33.3 (4.9) | 15.6 (7.9) |
| Hot conditions (n = 10) | 69.7 (9.5) | 18.0 (4.9) | 35.2 (3.3) | 14.0 (5.3) |
| Thermo-neutral conditions (n = 8) | 67.0 (11.9) | 12.9 (5.8) | 31.3 (5.7) | 17.4 (10.2) |
| Nurses (n = 5) | 65.6 (8.3) | 13.9 (3.9) | 33.4 (4.4) | 13.1 (2.2) |
| Physicians (n = 13) | 69.6 (11.1) | 16.5 (6.3) | 33.3 (5.3) | 16.6 (9.2) |
| Type of Event | Condition | No. of Events (Participants) | Donning, n | Doffing, n | PIV, n | MLC, n | ETI, n |
|---|---|---|---|---|---|---|---|
| Health-Assessment Trigger | Hot | 7 (4) | 0 | 0 | 0 | 4 | 3 |
| Thermo-neutral | 1 (1) | 0 | 0 | 0 | 0 | 1 | |
| Minor Breach | Hot | 26 (9) | 1 | 14 | 2 | 5 | 2 |
| Thermo-neutral | 21 (7) | 0 | 17 | 1 | 1 | 2 | |
| Near-Miss Incident | Hot | 21 (7) | 0 | 0 | 8 | 11 | 2 |
| Thermo-neutral | 23 (8) | 0 | 0 | 11 | 1 | 0 |
| Item | Study Changes | Rationale |
|---|---|---|
| Procedural tasks | Changes to the nurses’ procedural tasks | To align tasks with the expertise of acute care nurses, new tasks were developed (nasogastric tube insertion, urinary catheter insertion, administration of drugs via infusion pumps, and set-up of a CRRT machine). |
| Randomization | Stratified randomization | In the subsequent trial, randomization will be stratified by professional status (nurse vs. physician). |
| Cognitive tasks | Addition of objective assessment of stress effects | To objectively measure how heat stress affects HCWs’ cognitive function, we added tests of cognitive performance to complement subjective measures (i.e., post simulation questionnaire). Computer-based cognitive tasks will assess attention, decision-making, reaction time, learning, spatial memory, and working memory before and after the simulation. |
| Data collection tools | Addition of Instructor Guide | The Instructor Guide provides detailed instructions on CRF completion and defines grading criteria for each task item, thus reducing inter-rater variability. |
| Refinement of data tools | We eliminated redundant items from the CRF and questionnaires. | |
| Addition of video cameras | Multiple video cameras record the simulation and help data collectors to be accurate. | |
| Equipment | Equivital© for temperature measurement | The previous four skin thermistors to measure temperature required shaving participants and complex data computation. The simpler Equivital© device is now used. |
| Ihealth© to Omron© BP cuff | The Omron© BP cuff can function without Bluetooth while in the chamber, unlike Ihealth©. | |
| Chamber repairs | To ensure precise control of the temperature and humidity inside the climatic chamber. | |
| Monitoring participant safety | Eliminated pre-doffing vitals | Removal of pre-doffing vitals improved procedure flow and reduced task interruption. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiiza, P.; Mullin, S.I.; Teo, K.; Goodman, L.; Perez, A.; Pinto, R.; Thompson, K.; Piquette, D.; Hall, T.; Bah, E.I.; et al. Establishing Healthcare Worker Performance and Safety in Providing Critical Care for Patients in a Simulated Ebola Treatment Unit: Non-Randomized Pilot Study. Viruses 2021, 13, 2205. https://doi.org/10.3390/v13112205
Kiiza P, Mullin SI, Teo K, Goodman L, Perez A, Pinto R, Thompson K, Piquette D, Hall T, Bah EI, et al. Establishing Healthcare Worker Performance and Safety in Providing Critical Care for Patients in a Simulated Ebola Treatment Unit: Non-Randomized Pilot Study. Viruses. 2021; 13(11):2205. https://doi.org/10.3390/v13112205
Chicago/Turabian StyleKiiza, Peter, Sarah I. Mullin, Koren Teo, Len Goodman, Adic Perez, Ruxandra Pinto, Kelly Thompson, Dominique Piquette, Trevor Hall, Elhadj I. Bah, and et al. 2021. "Establishing Healthcare Worker Performance and Safety in Providing Critical Care for Patients in a Simulated Ebola Treatment Unit: Non-Randomized Pilot Study" Viruses 13, no. 11: 2205. https://doi.org/10.3390/v13112205