
Abstract
Introduction
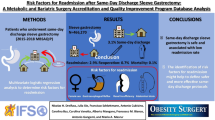
Decreasing the length of stay following bariatric surgery can reduce pressure on hospitals and surgical costs and increase patient satisfaction. We examine trends in length of hospital stay following bariatric surgery and in post-operative complications.
Methods and Procedures
The 2015–2019 Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP) database was used to compile patients undergoing Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy. Patients were categorized into either early discharge (within one day of surgery) or late discharge, and patient and non-patient factors were compared between the two groups. A multivariable logistic regression was carried out to determine predictive factors for early discharge.
Results
We evaluated 748,955 patients, with 399,918 (53%) being discharged early. Patients discharged early were younger and had fewer associated medical problems. The rate of early discharge increased between 2015 and 2019 (42.1% in 2015 vs 62.0% in 2019), while complication rates decreased or were unchanged. Multivariable analysis revealed lower ASA classification (OR 1.07; CI 1.06–1.09; p < 0.0001) and operative year (2019 vs. 2015 OR 2.26; CI 2.22–2.29; p < 0.0001) to be independently associated with early discharge. Several factors including undergoing RYGB (OR 0.44 CI 0.44–0.45; p < 0.0001), and dialysis dependence (OR 0.50; CI 0.45–0.55; p < 0.0001) among others, were associated with reduced early discharge likelihood.
Conclusions
There is a trend in bariatric surgery towards the practice of early discharge, which is safe for patients. Further work is needed to develop a set of criteria to determine which patients are best suited for this practice.
Graphical abstract


Similar content being viewed by others


References
Chang SH, Freeman NLB, Lee JA, et al. Early major complications after bariatric surgery in the USA, 2003–2014: a systematic review and meta-analysis. Obes Rev. 2018;19(4):529–37.
Arroyo-Johnson C, Mincey KD. Obesity epidemiology worldwide. Gastroenterol Clin North Am. 2016;45(4):571–9. https://doi.org/10.1016/j.gtc.2016.07.012.
Andolfi C, Fisichella PM. Epidemiology of obesity and associated comorbidities. J Laparoendosc Adv Surg Tech A. 2018;28(8):919–24. https://doi.org/10.1089/lap.2018.0380.
Frohman HA, Rychahou PG, Li J, et al. Development of murine bariatric surgery models: lessons learned. J Surg Res. 2018;229:302–10. https://doi.org/10.1016/j.jss.2018.04.022.
Jones DB, Abu-Nuwar MRA, Ku CM, et al. Less pain and earlier discharge after implementation of a multidisciplinary enhanced recovery after surgery (ERAS) protocol for laparoscopic sleeve gastrectomy. Surg Endosc. 2020;34(12):5574–82. https://doi.org/10.1007/s00464-019-07358-w.
Khorgami Z, Petrosky JA, Andalib A, et al. Fast track bariatric surgery: safety of discharge on the first postoperative day after bariatric surgery. Surg Obes Relat Dis. 2017;13(2):273–80. https://doi.org/10.1016/j.soard.2016.01.034.
Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292–8. https://doi.org/10.1001/jamasurg.2016.4952.
Waydia S, Gunawardene A, Gilbert J, et al. 23-hour/next day discharge post-laparoscopic Roux-en-Y gastric bypass (LRYGB) surgery is safe. Obes Surg. 2014;24(11):2007–10. https://doi.org/10.1007/s11695-014-1409-5.
Ban K, Berian J, Ko C. Does implementation of enhanced recovery after surgery (ERAS) protocols in colorectal surgery improve patient outcomes? Clin Colon Rectal Surg. 2019;32(2):109–13. https://doi.org/10.1055/s-0038-1676475.
Carmichael JC, Keller DS, Baldini G, et al. Clinical practice guidelines for enhanced recovery after colon and rectal surgery from the American Society of Colon and Rectal Surgeons and Society of American Gastrointestinal and Endoscopic Surgeons. Dis Colon Rectum. 2017;60(8):761–84. https://doi.org/10.1097/DCR.0000000000000883.
Meunier H, Le Roux Y, Fiant AL, et al. Does the implementation of enhanced recovery after surgery (ERAS) Guidelines improve outcomes of bariatric surgery? A propensity score analysis in 464 patients. Obes Surg. 2019;29(9):2843–53. https://doi.org/10.1007/s11695-019-03943-z.
American College of Surgeons. Metabolic and bariatric surgery accreditation and quality improvement program. 2021. https://www.facs.org/quality-programs/mbsaqip. Accessed 12 June 2021
Abraham A, Ikramuddin S, Jahansouz C, et al. Trends in bariatric surgery: procedure selection, revisional surgeries, and readmissions. OBES SURG. 2016;26:1371–7. https://doi.org/10.1007/s11695-015-1974-2.
Peterli R, Wölnerhanssen BK, Peters T, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss in patients with morbid obesity: the SM-BOSS randomized clinical trial. JAMA. 2018;319(3):255–65. https://doi.org/10.1001/jama.2017.20897.
Salminen P, Helmiö M, Ovaska J, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss at 5 years among patients with morbid obesity: the SLEEVEPASS randomized clinical trial. JAMA. 2018;319(3):241–54. https://doi.org/10.1001/jama.2017.20313.
Brockmeyer JR, Simon TE, Jacob RK, et al. Upper gastrointestinal swallow study following bariatric surgery: institutional review and review of the literature. Obes Surg. 2012;22(7):1039–43. https://doi.org/10.1007/s11695-012-0658-4.
Schiesser M, Guber J, Wildi S, et al. Utility of routine versus selective upper gastrointestinal series to detect anastomotic leaks after laparoscopic gastric bypass. Obes Surg. 2011;21(8):1238–42. https://doi.org/10.1007/s11695-010-0284-y.
Quartararo G, Facchiano E, Scaringi S, et al. Upper gastrointestinal series after Roux-en-Y gastric bypass for morbid obesity: effectiveness in leakage detection. a systematic review of the literature. Obes Surg. 2014;24(7):1096–101. https://doi.org/10.1007/s11695-014-1263-5.
Sakran N, Goitein D, Raziel A, et al. Gastric leaks after sleeve gastrectomy: a multicenter experience with 2,834 patients. Surg Endosc. 2013;27:240–5.
Carmichael J, Keller D, Baldini G, et al. Clinical practice guidelines for enhanced recovery after colon and rectal surgery from the American Society of Colon and Rectal Surgeons and Society of American Gastrointestinal and Endoscopic Surgeons. Dis Colon Rectum. 2017;60(8):761–84.
Matłok M, Pędziwiatr M, Major P, et al. One hundred seventy-nine consecutive bariatric operations after introduction of protocol inspired by the principles of enhanced recovery after surgery (ERAS®) in bariatric surgery. Med Sci Monit. 2015;21:791–7. https://doi.org/10.12659/MSM.893297.
Aryaie AH, Reddy V, Dattilo Z, et al. Safety of same-day discharge after laparoscopic sleeve gastrectomy: propensity score-matched analysis of the metabolic and bariatric surgery accreditation and quality improvement program registry. Surg Obes Relat Dis. 2021;17(1):46–53. https://doi.org/10.1016/j.soard.2020.08.039.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. As this was a retrospective study, formal consent was not required.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key Points
- Decreased admission length benefits the patient and healthcare system.
- From 2015 to 2019 rates of early discharge increased, and complications decreased.
- Early discharge is safe for bariatric patients.
- Further development of a criteria for patient selection is necessary.
Rights and permissions
About this article

Cite this article
Houlder, K., Mocanu, V., Verhoeff, K. et al. Trends, Outcomes, and Impact of Early Discharge Following Bariatric Surgery: a Retrospective MBSAQIP Analysis of 748,955 Patients. OBES SURG 32, 2572–2581 (2022). https://doi.org/10.1007/s11695-022-06108-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-022-06108-7