
Abstract
Purpose
Evidence of variation in mortality after surgery may indicate preventable postoperative death. We sought to determine if regional differences in outcome were present in surgical patients admitted to critical care in the UK.
Methods
We extracted data on admission characteristics, case mix and outcome of all patients admitted to UK critical care units following surgery for the calendar year of 2009. We also used publicly held data on regional population, volume of surgery and bed provision. Multilevel regression analysis was used to adjust for the effects of case mix and regional critical care bed provision on acute hospital mortality.
Results
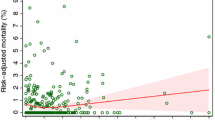
A total of 16,147 patients admitted to critical care following surgery were included in this analysis. Median odds ratio (MOR) was used to describe regional-level variance in acute hospital mortality. Significant variation was identified (MOR 1.14; 95 % CI 1.07, 1.28) and persisted following adjustment for case mix (MOR 1.10; 95 % CI 1.04, 1.25) and regional critical care bed provision (MOR 1.09; 95 % CI 1.04, 1.24). Critical care bed utilisation (surgical critical care admissions per 100,000 surgical procedures) seemed to better explain this observation (MOR 1.03; 95 % CI 1.00, 29.26) and was associated with statistically significant reduction in mortality (OR 0.91; 95 % CI 0.85, 0.97; p = 0.01).
Conclusion
Significant regional variation in hospital mortality for patients admitted to critical care following surgery was observed. Critical care bed utilisation seemed to better explain this observation and was associated with improved outcome.




Similar content being viewed by others


References
Weiser TG, Regenbogen SE, Thompson KD et al (2008) An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 372(9633):139–144
Khuri SF, Henderson WG, DePalma RG et al (2005) Determinants of long-term survival after major surgery and the adverse effect of postoperative complications. Ann Surg 242(3):326–341
Wang Y, Eldridge N, Metersky ML et al (2014) National trends in patient safety for four common conditions, 2005–2011. N Engl J Med 370:341–351
Bennett-Guerrero E, Hyam JA, Shaefi S et al (2003) Comparison of P-POSSUM risk-adjusted mortality rates after surgery between patients in the USA and the UK. Br J Surg 90:1593–1598
Symons NR, Moorthy K, Almoudaris AM et al (2013) Mortality in high-risk emergency general surgical admissions. Br J Surg 100:1318–1325
Saunders DI, Murray D, Pichel AC, Varley S, Peden CJ, On behalf of the members of the UK Emergency Laparotomy Network (2012) Variations in mortality after emergency laparotomy: the first report of the UK Emergency Laparotomy Network. Br J Anaesth 109:368–375
Pearse RM, Moreno RP, Bauer P et al (2012) Mortality after surgery in europe: a 7 day cohort study. Lancet 380:1059–1065
Ghaferi AA, Birkmeyer JD, Dimick JB (2009) Variation in hospital mortality associated with inpatient surgery. N Engl J Med 361:1368–1375
Aylin P, Alexandrescu R, Jen MH, Mayer EK, Bottle A (2013) Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. doi:10.1136/bmj.f2424
Finks JF, Osborne NH, Birkmeyer JD (2011) Trends in hospital volume and operative mortality for high-risk surgery. N Engl J Med 364:2128–2137
Wunsch H, Angus DC, Harrison DA et al (2008) Variation in critical care services across North America and Western Europe. Crit Care Med 36:2787–2793
Jhanji S, Thomas B, Ely A, Watson D, Hinds CJ, Pearse RM (2008) Mortality and utilisation of critical care resources amongst high-risk surgical patients in a large NHS trust. Anaesthesia 63:695–700
The General Register Office (Scotland) (2010) Mid-2009 population estimates Scotland population estimates by sex, age and administrative area. ONS, Edinburgh
The Office for National Statistics (2010) Population estimates for UK, England and Wales, Scotland and Northern Ireland, mid 2009. http://www.ons.gov.uk/ons/publications/re-reference-tables.html?edition=tcm%3A77-213645. Updated 2010. Accessed 26 Feb 2012
Eddleston J, Goldhill D, Morris J (2009) Levels of critical care for adult patients. Intensive Care Society Standards, London
Larsen K, Merlo J (2005) Appropriate assessment of neighborhood effects on individual health: integrating random and fixed effects in multilevel logistic regression. Am J Epidemiol 161:81–88
Merlo J, Chaix B, Yang M, Lynch J, Råstam L (2005) A brief conceptual tutorial of multilevel analysis in social epidemiology: linking the statistical concept of clustering to the idea of contextual phenomenon. J Epidemiol Community Health 59:443–449
Hamilton MA, Cecconi M, Rhodes A (2011) A systematic review and meta-analysis on the use of preemptive hemodynamic intervention to improve postoperative outcomes in moderate and high-risk surgical patients. Anesth Analg 112:1392–1402
Pearse R, Dawson D, Fawcett J, Rhodes A, Grounds RM, Bennett ED (2005) Early goal-directed therapy after major surgery reduces complications and duration of hospital stay. A randomised, controlled trial. Crit Care 9:R687–R693
Information Services Division (2007) NHS hospital data quality: towards better data from Scottish hospitals. Scottish Executive Health Department, Edinburgh
Young MJ, Lenhart J, Wasser TE et al (1999) Evidence for the Will Rogers phenomenon in migration of employees to managed care plans. Ann Intern Med 14(9):564–566
Appleby J, Raleigh V, Frosini F, Bevan G, Gao H, Lyscom T (2011) Variations in health care: the good, the bad and the inexplicable. The King’s Fund, London
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
MG holds a Chief Scientist Office (Scotland) NHS Research Scheme Fellowship. RP reports grants and personal fees from Nestle Health Sciences, personal fees from Massimo Inc., personal fees from Edwards Life Sciences, and equipment loans from LiDCO Ltd. The other authors confirm they have no conflict of interest.
Sources of funding
MG holds a research fellowship from the Chief Scientist’s Office, Scotland.
Additional information
Take-home message: Regional variation in mortality for patients admitted to ICU after high-risk surgery exists within a uniform healthcare system and persists after adjustment for case mix. Variation in absolute regional provision of intensive care beds (ICU beds per 100,000 population) did not appear to explain this finding; ICU bed utilisation (ICU admissions per 100,000 surgical procedures) better explains the observed variation and is associated with improved outcome.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Gillies, M.A., Power, G.S., Harrison, D.A. et al. Regional variation in critical care provision and outcome after high-risk surgery. Intensive Care Med 41, 1809–1816 (2015). https://doi.org/10.1007/s00134-015-3980-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-015-3980-1